By Victoria Wilson | 10 July 2026
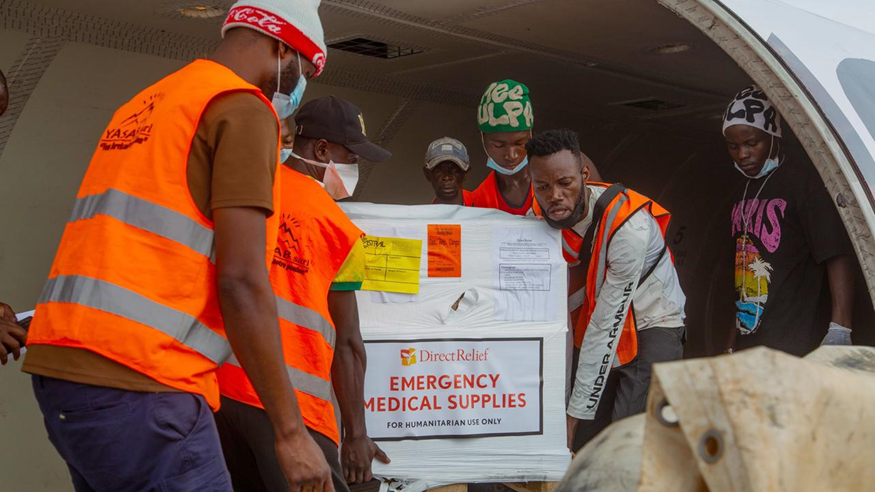
Africa CDC flagged PPE shortages in Bunia on the second day of the outbreak response in May; striking health workers have also cited inadequate protective equipment among their demands. Photo: Castro WML Studio / Direct Relief
More than 600 people have died in the Democratic Republic of the Congo from the Bundibugyo Ebola strain as of 9 July, more than double the 254 deaths documented on 21 June. The outbreak has spread from three provinces to five, has been confirmed in France, and was still accelerating as of 8 July, when 51 new cases and 20 deaths were recorded in a single 24-hour period. DRC Health Minister Roger Kamba stated on 9 July that the peak has not been identified.
The epidemiological surveillance teams, burial workers, and community outreach staff responsible for tracking the spread in Bunia have not received wages since the outbreak was declared on 15 May. On 7 July they walked off the response. “We might have to give up our jobs,” said Dr. Ben Bakule, a community investigator in Ituri Province. “These are risks we’re taking. We risk dying for nothing.”
A letter to Ituri’s governor, dated 5 July, stated that months of unpaid service had produced “significant socio-economic difficulties.”
THE NUMBERS, SIX WEEKS ON
As of 23 June, 254 people had died and 1,003 cases had been confirmed. As of 9 July, the confirmed case count stands at 1,759. As of 19 June, seventeen healthcare workers had died and 75 had been infected. Case fatality is running at approximately 34 percent, consistent with prior Bundibugyo outbreaks.
MSF has expanded its deployment to 1,400 staff across seven treatment centres in DRC and Uganda. Treatment centres are operating at 94 percent bed occupancy.
China has sent two expert teams to Kinshasa. A five-member mission that arrived on 2 June is on a three-month deployment covering epidemiology, clinical diagnosis, and laboratory support. A second team of six specialists arrived on 3 July with a specific mandate to strengthen local diagnostic testing capacity. DRC President Félix Tshisekedi acknowledged China’s contribution on 2 July.

China’s National Health Commission deployed the first team on 2 June; a second six-member team followed on 3 July with a specific focus on strengthening local laboratory and diagnostic capacity. Photo: Xinhua
FIVE PROVINCES
Three provinces carried confirmed cases when the response began: Ituri, North Kivu, and South Kivu. Two more have since been added.
The outbreak reached Tshopo province through patient movement toward Kisangani, the provincial capital. One confirmed case was traced to a pregnant woman who died in Bunia and was transported to Kisangani by family members. Al Jazeera has reported two further unconfirmed cases in Kisangani that appear to have no geographic link to the outbreak epicentre, suggesting the virus may be circulating in the city through an undocumented transmission chain. Haut-Uele province was added through patient movement toward the Wamba area.
Ituri remains the epicentre with more than 1,600 confirmed cases. North Kivu continues to see active case increases. South Kivu alone has recorded no new cases since 26 May.
The outbreak has also crossed continents. One case was confirmed in France on 24 June. A US citizen was medically evacuated to Germany in May. Uganda, which confirmed 20 cases and 2 deaths in June, has recorded no new cases since 21 June, with all cases in Kampala and no documented community spread.

Tshopo and Haut-Uele were not part of the outbreak when it was declared in May; both have been reached through patient movement out of Ituri. Map: Chaotic Enby / Wikimedia Commons (CC BY-SA 4.0)
STRIKE IN THE EPICENTRE
In the absence of an approved vaccine or treatment for the Bundibugyo strain, the response depends on contact tracing: identifying exposed individuals, placing them under surveillance, and interrupting transmission before symptoms appear. The workers on strike in Bunia and Rwampara are the ones who conduct it.
“Since the Ebola virus disease outbreak was declared, we’ve been demanding payment for our work,” said Dr. Biensi Kano, a member of Bunia’s epidemiological surveillance committee. “We are working day and night without being paid,” said Dr. Ghislain Maneba, an epidemiologist at the Rwampara health zone.
The reason offered by Akilimali Pierre, incident manager at the National Institute of Public Health, is an airport closure that has impeded the flow of funds to the response.
THE TRIAL AND THE GAP
The PARTNERS clinical trial launched on 2 July at the Evangelical Medical Center in Bunia. It is testing three candidate treatments: remdesivir and the monoclonal antibody MBP134 for confirmed cases, and obeldsivir as post-exposure prophylaxis for contacts. Results are expected in three to six months.
Of the US$26 million needed to fund the trial fully, US$10 million has been secured. Africa CDC Director-General Dr. Jean Kaseya stated: “We have the science. We now need the funding to use it. Every day of delay costs lives we could save.” Of the US$319 million required for the full response, US$287 million remains unsecured.
Identifying patients for the trial requires contact tracers to track every exposure. The workers responsible for that network in Bunia are on strike because have not been paid in 56 days.